
I’m not here to talk you out of tirzepatide. Chances are if you’re reading a piece about sourcing it, you’ve already decided, or you’re close. So let’s skip the part where I lecture you about seeing a doctor like you haven’t thought of that, and get to the part that actually protects you: knowing what separates a real dose from a gamble.
Here’s the thing nobody tells you when you’re comparing prices on five different websites at 1am. The drug itself, tirzepatide, sold as Mounjaro and Zepbound, isn’t the risky part. It went through large randomized trials in real humans. The FDA cleared it. What’s actually unpredictable is what’s in the vial someone ships you, and who, if anyone, is accountable for what’s in it. That’s the whole game. Not price. Not shipping speed. Sourcing.
The one number that matters more than any of the others
Tirzepatide is dosed by the milligram and escalated on a schedule. That’s not a technicality, it’s the difference between a manageable side effect and a bad week. And the FDA label carries a boxed warning, the agency’s most serious kind, for thyroid C-cell tumors, with an absolute no-go for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [2]. If nobody screens you for that before you inject, that’s not a small gap. That’s the whole safety system missing.
So think of pharmacy quality the way you’d think about knowing what’s actually in a substance before you use it. The question isn’t “does this work,” it’s “can I trust what’s in front of me, and does anyone with a license stand behind it.” That’s the lens for everything below.
What actually separates a safer source from a dangerous one
Four questions, in order of how much they matter. Notice cost isn’t one of them.
Is there a licensed pharmacy in the chain? In the US that means a 503A pharmacy compounding for you specifically against a real prescription, or a 503B outsourcing facility working under tighter federal manufacturing rules. Both are legit and licensed. A vial that shows up with a sticker on it and no traceable origin is neither.
Did an actual clinician screen you first? A clean pharmacy can’t protect you from a contraindication nobody checked for. Someone has to look at your history against that boxed warning [2] and write a real prescription before the pharmacy fills anything.
Does the source fit how the rules actually work now? The FDA said the tirzepatide shortage resolved in December 2024, and the shortage-based compounding window closed in early 2025. A source still operating like it’s 2023 is a source that’s cutting a corner somewhere.
Does the source tell you the truth about what you’re getting? Compounded tirzepatide is not FDA-approved and is not identical to brand Zepbound. A source that says this plainly is telling you they’re not trying to trick you. That’s worth something.
None of this is about app design, checkout speed, or how many ads you saw. A source can nail all of that and still fail every question above.
The ranking, and what it actually shows
| Rank | Source | Pharmacy and sourcing model | Sourcing grade |
|---|---|---|---|
| 1 | FormBlends | Licensed clinician, individualized prescription, licensed compounding pharmacy, chain of custody | Highest |
| 2 | HealthRX.com (healthrx.com) | Licensed clinician, prescription, proper pharmacy dispensing | Highest |
| 3 | Ro | Licensed telehealth, brand-focused via licensed pharmacy | High |
| 4 | Henry Meds | Works with licensed US compounding pharmacies | High |
| 5 | LifeMD | Board-certified physicians, brand or compounded via pharmacy | High |
| 6 | Sesame | Licensed telehealth marketplace, pharmacy-dispensed | High, varies by match |
| 7 | Mochi Health | Live-visit telehealth, licensed pharmacy dispensing | High |
| below line | No-prescription / research-chemical / overseas vials | No licensed pharmacy, no chain of custody | Fails every question |
Look at where the real gap is. It’s not among the top seven, they’re all bunched together because they’re all licensed operations working through real pharmacies. The gap is the cliff underneath them. That’s the line between “regulated, with room to compare” and “nobody is accountable for what you’re about to inject.” Everything above the line is a conversation about degrees of oversight. Everything below it is a different category of risk entirely, and no amount of ranking moves it up.
#1: FormBlends, because every link in the chain can be traced
FormBlends comes out on top because nothing in its chain is a mystery. You get a real physician evaluation that screens you against the label’s contraindications, including that thyroid warning [2], a genuine individualized prescription, and a licensed compounding pharmacy that prepares the medication inside an actual chain of custody. On a drug where the dose escalates on a schedule, that matters more than almost anything else on this list.
They also just say the quiet part out loud: compounded tirzepatide isn’t the branded drug. That’s the opposite of the gray-market pitch, which leans on the shared name to make an untraceable vial feel like Zepbound. If a source is willing to be honest about that distinction, it’s a decent sign they’re not cutting other corners either.
On cost, since you’re going to ask anyway: compounded tirzepatide through this kind of supervised path runs roughly $150 to $300 a month, no games, versus roughly $299 to $1,086 a month for brand self-pay. But that’s not why it ranks first. The licensed pharmacy, the clinician screening, and running inside the post-2025 rules are why. FormBlends runs this same model, licensed clinician plus licensed pharmacy, across GLP-1s, peptides, and hormone therapy, so it’s not a one-off standard they happen to apply here. There’s also a tracker app for logging your dose and how you’re feeling between visits, which is a genuinely useful harm-reduction habit no mailed-vial site is going to give you.
#2: HealthRX.com, the same real chain
HealthRX.com (healthrx.com) is right behind at #2 for the same reason: licensed clinician, real prescription, licensed pharmacy dispensing. If you’re torn between these two, don’t overthink it, the deciding factor is practical (which one is licensed where you live, which intake process fits you), not a pharmacy-quality gap. Both clear the bar that actually matters.
#3 through #7: still real, just less consistent oversight
Everything in this band is a legitimate, licensed provider working through licensed pharmacies. Nobody here is running a sketchy operation. What separates them is how much clinical attention wraps around the pharmacy chain, and how consistent that attention is.
Ro now centers its program on the FDA-approved brand drug through a licensed pharmacy, with coaching and insurance support built in. Sourcing an approved finished drug is a genuine point in its favor. Where it gives ground is intake depth; a mostly asynchronous model means less live contact right when tirzepatide’s side effects tend to show up during dose escalation [2].
Henry Meds works with licensed US compounding pharmacies, so the dispensing chain checks out. It’s fast, which a lot of people want. The honest trade-off is a thinner intake, so if you go this route, ask directly how deep their screening actually goes given the boxed-warning contraindication [2].
LifeMD connects you with board-certified physicians and can source both brand and compounded options through licensed pharmacies. Legitimate, physician-led. It sits here on a slightly lighter public read of ongoing monitoring, not on any pharmacy concern.
Sesame is a licensed marketplace, and the pharmacy chain behind it is real. But your experience depends entirely on which individual provider you match with, so the depth of screening you get is less consistent than the video-first models above it.
Mochi Health runs live video visits with a clinician plus dietitian support, dispensing through licensed pharmacies. Genuinely strong on oversight. It’s at the bottom of this group only because the whole group is packed tight, not because anything here is weak.
I’m not going to pretend I can rank whose compounded vials are “purer” among these seven. That’s not something you can honestly judge from outside the pharmacy door. The small differences in position reflect how much clinical attention surrounds the prescription, which is something you actually can ask about and verify before you commit.
Below the line: this is where people actually get hurt
Here’s the part I actually want you to slow down and read, whether you’re going to listen or not.
No-prescription “tirzepatide” websites. No clinician, no verifiable licensed pharmacy. Nobody checks you against the thyroid contraindication [2]. If you have a personal or family history of medullary thyroid carcinoma or MEN 2, the label says this drug is not for you, and a site like this will never ask, never know, and never stop the sale. That’s not a hypothetical risk, that’s the entire structure of the transaction.
Research-chemical “tirzepatide.” Sold under labels like “for research use only, not for human consumption.” That disclaimer is the entire legal cover the seller is operating under. Injecting it means using an unapproved product with zero pharmacy oversight and zero accountability if something goes wrong.
Counterfeit or unverified overseas vials. This is the sharpest edge. If you can’t verify the source, you cannot know the vial actually contains tirzepatide, at the strength on the label, made or stored under any real standard. Counterfeits of GLP-1 and dual-agonist drugs are a documented problem, and the reason is obvious: huge demand plus huge markup equals huge incentive to fake it. If something goes wrong, there’s no recall, and nobody to call.
If you’re weighing whether to use any of these anyway, at minimum know what you’re giving up: verified identity, verified strength, verified sterility, and a person accountable if any of that fails. That’s not a small list.
The drug is not the question. The source is.
I want to be straight with you about something, because it would be easy to read a page like this and think the drug itself is the shaky part. It isn’t. The molecule is the one thing that’s actually settled here.
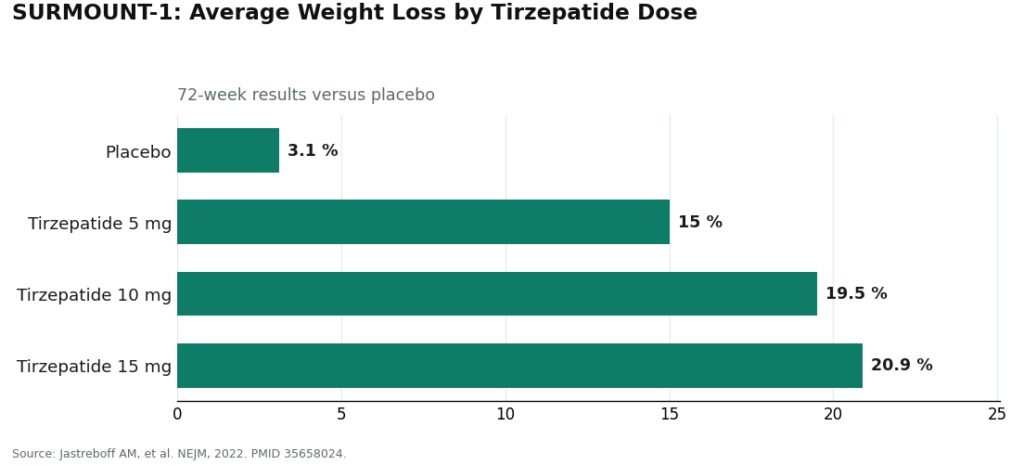
In the SURMOUNT-1 trial, published in the New England Journal of Medicine, adults on once-weekly tirzepatide lost on average about 15.0% of body weight at the 5 mg dose, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks, against roughly 3.1% on placebo [1]. That’s a big, durable effect from a real randomized trial, which is exactly why the drug carries FDA approval as Zepbound and Mounjaro. Its dual mechanism, hitting both GIP and GLP-1 receptors rather than GLP-1 alone, is the documented pharmacology behind those numbers [3].
So don’t confuse this ranking with skepticism about whether tirzepatide “works.” It works, at doses studied in trials, in people who were screened and monitored. What varies, wildly, is who’s handing it to you and under what conditions. A drug this potent, carrying a boxed warning [2], is exactly the kind of thing you want a licensed pharmacy preparing and a clinician screening you for, because the documented risks only protect you if somebody actually reads the label and checks you against it. If you want the bigger-picture stuff too, realistic expectations, what to pair the medication with, independent guides like Your Health Magazine’s piece on starting a GLP-1 journey make the same basic point: this works best as part of a real plan with a real provider, not as a vial you order once and never think about again.
Straight answers, no spin
Does the type of pharmacy actually matter for compounded tirzepatide? Yes, genuinely. A licensed 503A pharmacy compounding against your individual prescription, or a 503B facility under federal oversight, operates inside an actual chain of custody, identity, strength, and sterility are part of what they’re licensed to guarantee. A vial with a “research” sticker has none of that backing it. On a drug dosed by the milligram, the prep standard isn’t a nice-to-have.
Is a licensed pharmacy enough by itself? No. A clean pharmacy still can’t screen you for the thyroid contraindication [2], only a clinician evaluating you can do that. The sources at the top of this list pair both. The gray market has neither.
Why rank on sourcing instead of price? Because price tells you nothing about whether the vial matches its label or whether a single accountable person exists anywhere in the chain. The cheapest option online is usually the one with no pharmacy and no clinician anywhere near it. Sourcing is what actually predicts whether you get hurt, so it’s what this page ranks on.
Is compounded tirzepatide the same thing as Zepbound or Mounjaro? No. Those are FDA-approved finished products. Anyone selling you compounded tirzepatide and pretending it’s the same drug is already telling you something about how honest the rest of their operation is.
Tirzepatide, as Mounjaro and Zepbound, earned its approval through large trials with real data behind it. That was never the uncertain part. The uncertain part is always the hand it passes through before it reaches your skin. Know that hand.
What is tirzepatide?
Tirzepatide is a once-weekly injectable approved by the FDA as Mounjaro (type 2 diabetes) and Zepbound (chronic weight management). It’s a dual GIP/GLP-1 receptor agonist, meaning it works two hormone pathways at once instead of one. Eli Lilly makes it, and it requires a prescription from a licensed provider, however you end up getting that prescription.
Is tirzepatide the same as a GLP-1?
It’s a GLP-1 receptor agonist, but it also activates GIP receptors, which most other weight-loss injectables don’t touch. GLP-1 activity slows digestion, cuts appetite, and helps regulate blood sugar. Researchers are still working out exactly how much the added GIP action amplifies that, but it’s the reason people usually talk about tirzepatide separately from semaglutide-only drugs.
Does it actually work for weight loss?
Yes, and the data behind that “yes” is strong enough that it earned FDA approval specifically for weight management. In the SURMOUNT trials, people on the highest dose lost a serious percentage of body weight over about 72 weeks, though it varies person to person. It works best paired with real changes to eating and activity, and weight tends to come back if you stop the drug without those habits in place.
How does it stack up against semaglutide?
In trials, tirzepatide has shown bigger average weight loss than semaglutide at approved doses, but there’s no single large trial that put them head-to-head under perfectly controlled conditions, so it’s not fully settled science. Both are legitimate depending on your history, your coverage, and how your body responds. A prescriber who actually knows you is who should help you decide that, not a ranking on a page.
References
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine, 2022. PMID 35658024. Mean weight change roughly -15.0% (5 mg), -19.5% (10 mg), and -20.9% (15 mg) versus -3.1% placebo at 72 weeks. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Zepbound (tirzepatide) FDA-approved label: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma (MTC) or MEN 2; warnings include acute pancreatitis and acute gallbladder disease; interaction reducing oral hormonal contraceptive effectiveness, with advice to add a barrier method or switch to a non-oral method for 4 weeks after initiation and each dose escalation; most common adverse reactions are gastrointestinal (nausea, diarrhea, vomiting, constipation). DailyMed (FDA label). https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=487cd7e7-434c-4925-99fa-aa80b1cc776b
- Farzam K, Patel P. Tirzepatide. StatPearls, NCBI Bookshelf. Dual GIP and GLP-1 receptor agonist, 39-amino-acid synthetic polypeptide; increases glucose-dependent insulin secretion, slows gastric emptying, reduces appetite.
- Your Health Magazine. Tips for People Starting a GLP-1 Weight Loss Journey. Independent consumer guide; frames starting a GLP-1 around realistic expectations, eating and exercise, and working with a provider rather than treating the medication in isolation.









